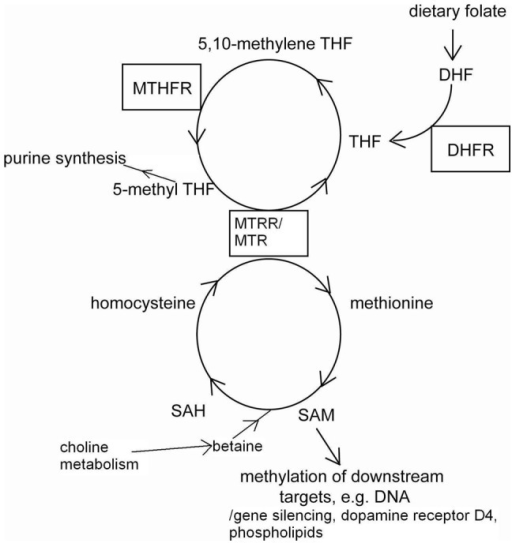
What happens when we ingest methylcobalamin? Unfortunately, it doesn't seem to go straight to where it might be needed in the body. A complex processing of B12, which is still the subject of investigation, happens in the cells first. (https://www.ncbi.nlm.nih.gov/pmc/articles/PMC4692085/, https://www.ncbi.nlm.nih.gov/pubmed/27771510) Methylcobalamin, adenosylcobalamin, and cyanocobalamin all undergo separation of the non-cobalamin part from the cobalamin part by the protein MMACHC. MMACHC catalyzes the decyanation of cyanocobalamin and the dealkylation of methylcobalamin and adenosylcobalamin, after which the cobalamin is chaperoned (cobalamin is very volatile on its own) and changed to adenosylcobalamin and methylcobalamin. The transformation of cobalamin to methylcobalamin, based on recent findings, appears to be part of an interplay of several proteins, including both MMACHC and methionine synthase (MS). (https://www.ncbi.nlm.nih.gov/pubmed/27771510) In other words, a problem with MS could not only affect MS in its homocysteine-salvaging function but could also make MeCbl less available to due to MS interacting with MMACHC, which decyanizes cyanocobalamin.
If you've ever read about chaos theory, you probably saw a mention of feedback loops. Feedback loops are an important principle to understand when dealing with systems of complex interactions such as those involving MS and B12 transport, conversion, and use.
The term feedback refers to a situation in which two (or more) dynamical systems are connected together such that each system influences the other and their dynamics are thus strongly coupled. Simple causal reasoning about a feedback system is difficult because the first system influences the second and the second system influences the first, leading to a circular argument. This makes reasoning based on cause and effect tricky, and it is necessary to analyze the system as a whole. A consequence of this is that the behavior of feedback systems is often counterintuitive.
http://authors.library.caltech.edu/25062/1/Feedback08.pdf (Feedback Systems: An Introduction for Scientists and Engineers. Karl Johan Åström; Richard M. Murray (2010). "§1.1: What is feedback?" Princeton University Press, p. 1).
I'm not going to try to untangle exactly what is happening between cyanocobalamin, MMACHC, and MS in the human brain, for we lack the necessary knowledge to do so at present. But we have evidence from a paper published last year that the fetal brain, for whatever reason, doesn't break down cyanocobalamin as well as expected.
We found CNCbl to be 15-fold higher in fetal samples, as compared to 0–20 yr old subjects, suggesting unique Cbl metabolism during fetal development. However, the underlying cause of this higher CNCbl level remains unclear, as does the biological origin CNCbl. Maternal folate and vitamin B12 supplementation is a common recommendation during pregnancy, which could be a source of the elevated CNCbl we observed, although Cbl levels in placenta were comparatively low. Conversion of CNCbl to active cofactors MeCbl and AdoCbl requires NADPH- or GSH-dependent decyanation by MMACHC and it is possible that the developing fetal brain has diminished decyanation capacity. The markedly higher level of inactive CNCbl could potentially have functional consequences by competing with MeCbl and AdoCbl, restricting their cofactor activity.
http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0146797 (references omitted).
An excess of CnCbl in the developing fetal brain could be restricting MeCbl activity? Which would negatively affect MS activity? That's exactly what we don't want to have happen if MS dysfunction is behind autism spectrum disorders.
Too little B12 in the brain has been linked to autism. (http://journals.plos.org/plosone/article?id=10.1371/journal.pone.0146797) And so has an excess of B12, according to the Johns Hopkins findings last year that I mentioned in a previous blog post: "Very high vitamin B12 levels in new moms are also potentially harmful, tripling the risk that her offspring will develop an autism spectrum disorder." (http://www.jhsph.edu/news/news-releases/2016/too-much-folate-in-pregnant-women-increases-risk-for-autism-study-suggests.html) The high B12 levels in the Johns Hopkins study population were almost certainly a result of cyanocobalamin in prenatal vitamins and fortified foods, for naturally occurring B12 forms are unlikely to be consumed at sustained excessively high levels unless one frequently eats clams and liver. (https://ods.od.nih.gov/factsheets/VitaminB12-HealthProfessional/).
Here's the worst part of the finding from the Johns Hopkins study: "If both levels [folate and B12] are extremely high, the risk that a child develops the disorder increases 17.6 times." (http://www.jhsph.edu/news/news-releases/2016/too-much-folate-in-pregnant-women-increases-risk-for-autism-study-suggests.html)
Talk about synergy! Yes, that said 17.6 times the risk of an autism spectrum disorders for children of women who had blood containing too much folate and B12, which almost certainly came from folic acid and cyanocobalamin in their prenatal vitamins and their fortified foods. Both the conscientious mothers who take their prenatal vitamins dutifully and economically disadvantaged mothers who rely on WIC--which generally limits their cereal choices to those that are highly fortified with folic acid and cyanocobalamin--are at risk of having excessive folate and B12, so their children end up at much greater risk of autism spectrum disorders, which are disorders of development, meaning it will be difficult or impossible to fully repair the damage later in life.
The heavy use of folic acid and cyanocobalamin, especially in conjunction, appears to have helped cause the dramatic rise in autism spectrum disorders in the last three decades. Folic acid and cyanocobalamin should be replaced with other forms of folate and B12 that are bioidentical to naturally, commonly occurring forms in order to minimize the hazard of causing unintended problems as has apparently happened with autism spectrum disorders. (I think ADHD is related to this mess, too--https://www.ncbi.nlm.nih.gov/pubmed/27346490--but I'll stay focused on autism for now.)
**This is one of a series of posts. Here are the links to each entry in the series.**
Introduction
Part 1
Part 2
Part 3
Part 4
Conclusion